Colposuspension
Stress urinary incontinence (SUI), referring to ‘involuntary loss of urine on effort or physical exertion, or on sneezing or coughing‘, is the most common type of urinary incontinence, affecting over 10-20% of women.
When SUI severely affects quality of life and conservative measures fail IUGA Non-Surgical_Approaches_to_Managing_Bladder_Problems, surgery may be considered.
Amongst the currently available surgical treatment options , colposuspension has been an effective and safe surgical treatment for SUI for more than half a century .
In recent years, due to negative media reports covering class actions concerning the use of mesh in surgical management of pelvic organ prolapse and urinary incontinence https://www.ausdoc.com.au/opinion/what-judge-got-wrong-transvaginal-mesh-device-scandal, more and more women are looking for non-mesh treatment options for
stress urinary incontinence. Colposuspension is such a procedure.
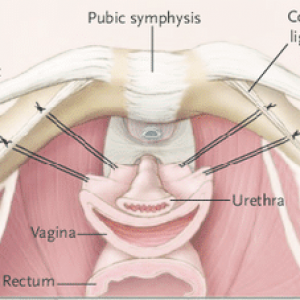
The procedure does not use mesh. Rather, after opening into the retropubic space, the surgeon places a series of sutures into the endopelvic fascia of the anterior vaginal wall to elevate and stabilise the proximal urethra and bladder neck to the pectineal ligament (Cooper’s ligament).
Initially done through a laparotomy, colposuspension can be performed through minimally invasive (keyhole) surgery using laparoscopic or robotic surgery in the hands of appropriately trained surgeons.
Associate Professor Alan Lam was one of the pioneering surgeons to perform and introduce laparoscopic colposuspension to Australia in the early 1990’s. He has taught many surgeons around the world about laparoscopic colposuspension and pelvic floor reconstructive surgery over the years.
For more information, go to:
RANZCOG Stress-Urinary-Incontinence
ACSQH Patient-information-resource-transvaginal-TV-mesh-Stress-Urina…